
Getting lip fillers is a popular way to enhance your smile, but it comes with rare, yet serious risks. The most critical complication you need to be aware of is vascular occlusion (VO). When a blood vessel is blocked during or after an injection, it cuts off the vital blood supply to your lips and surrounding skin.
Without immediate treatment, this lack of oxygen can lead to tissue death (necrosis) and permanent scarring. The key to a full recovery is recognizing the signs instantly and seeking urgent medical care.
If you recently had lip filler, check for these immediate red flags. Do not wait for these to resolve on their own.
- Intense, Escelating Pain: Pain that is sharp, throbbing, or worsens over time.
- Blanching (White/Pale Skin): The skin looks unusually white, gray, or dusky.
- Sluggish Capillary Refill: Press the affected area firmly for a few seconds. If it takes longer than 3 seconds for the pink color to return, blood flow is compromised.
- Temperature Drop: The affected lip or skin feels noticeably colder than the rest of your face.
What Is Vascular Occlusion in Lip Filler?
Vascular occlusion occurs when dermal filler interferes with the normal blood flow through an artery or vein. This happens in one of two ways:
- Direct Intravascular Injection: The needle or cannula accidentally punctures a blood vessel, and filler is injected directly inside, instantly acting like a plug.
- External Compression: Even if the filler does not enter the vessel, injecting too much product (a large bolus) into a tight space can press down heavily on a nearby artery. This external pressure crushes the vessel and chokes off the blood supply.
Important Note on Filler Types: Not all fillers are the same in an emergency. Hyaluronic acid (HA) fillers are the safest choice because they can be rapidly dissolved using an enzyme called hyaluronidase. Biostimulatory fillers (like calcium hydroxylapatite) cannot be dissolved, making occlusion treatment much more difficult.
Early Warning Signs & The Symptom Timeline
Recognizing vascular occlusion can be tricky because early symptoms are often mistaken for normal post-procedure discomfort. Furthermore, because many lip fillers contain lidocaine (a numbing agent) or epinephrine, the initial pain and whitening might be temporarily masked.
Symptoms can appear instantly while you are still in the chair, or they may develop up to 24 hours after your procedure.
Watch for this progression of symptoms:
Phase 1: Blanching and Pain (Immediate to 2 Hours)
- Blanching: The skin suddenly turns white or pale. This happens because the oxygen-rich blood is no longer reaching the surface.
- Severe Pain: A sharp, disproportionate pain that feels vastly different from the typical “pinch” of an injection.
Phase 2: Livedo Reticularis / Mottling (2 to 24 Hours)
- As deoxygenated blood pools in the tissue, the skin takes on a distinct, lacy, purple or bluish pattern known as livedo reticularis.
- Unlike a normal bruise, this mottled area often spreads along the path of the blocked artery, sometimes reaching up toward the nose.
Phase 3: Blisters and Pustules (24 to 72 Hours)
- If blood flow is not restored, the starving tissue begins to break down. Small white blisters or pustules will start forming on the surface of the skin. This is a severe warning sign that tissue death is imminent.
Phase 4: Tissue Necrosis (Days)
- The skin begins to die, turning black or forming hard, dark scabs (eschar). At this stage, irreversible scarring is highly likely. However, if high-dose hyaluronidase is administered within the first 48 hours, the chances of a full recovery remain very high.
Normal Swelling & Bruising vs. Vascular Occlusion
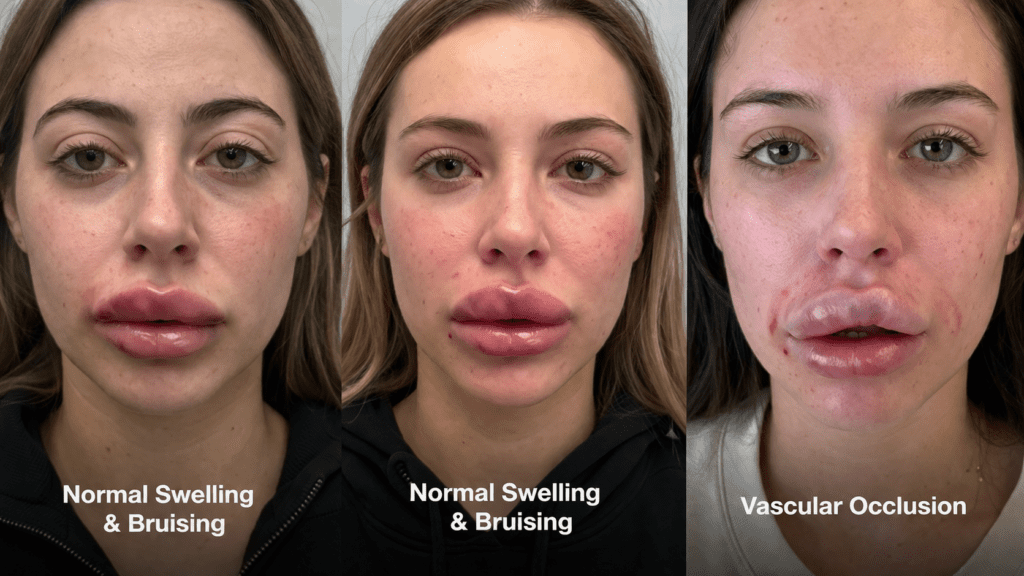
It is normal to experience some swelling, tenderness, and bruising after lip fillers. Use this clinical comparison table to determine if what you are experiencing is normal healing or a vascular emergency. Lip filler swelling stages is normal for everyone.
| Clinical Feature | Normal Swelling & Bruising | Vascular Occlusion (Emergency) |
| Pain Level | Mild to moderate tenderness; improves over time. | Intense, sharp, or escalating pain that throbs. |
| Skin Color | Redness, or localized blue/purple bruises. | White/pale (blanching), gray, or a “lacy” purple pattern. |
| Capillary Refill | Normal (Color returns in 1-2 seconds after pressing). | Delayed or Absent (Takes more than 3 seconds). |
| Skin Temperature | Normal or slightly warm due to inflammation. | Noticeably cool or cold to the touch. |
| Bruise Behavior | Stays localized to the needle entry point. | Spreads rapidly, often moving away from the injection site. |
Why Does Vascular Occlusion Happen? (Causes & Risk Factors)
Vascular occlusion is rare, but certain factors significantly increase the risk. It is rarely intentional, but rather a combination of human error, technique, and your unique facial anatomy.
1. Incorrect Injection Technique
The most common cause of a blocked vessel is placing the filler in the wrong tissue plane. Risk increases when an injector:
- Uses Sharp Needles Instead of Cannulas: Sharp needles can easily pierce an artery wall, whereas blunt-tipped cannulas tend to push vessels aside.
- Injects Under High Pressure: Forcing the filler in too fast doesn’t give the tissue time to adjust, increasing the chance of it shooting into a vessel.
- Fails to Aspirate: Aspiration is a safety check where the injector pulls back on the syringe plunger before injecting. If blood enters the needle, they know they are in a vessel and must reposition.
2. The Danger of “Too Much, Too Soon” (External Compression)
You don’t need a needle to enter a vein to cause an occlusion. If an injector places a massive amount of filler (a large bolus) directly on top of or next to a blood vessel, the heavy filler can physically crush the artery.
Prevention Pro-Tip: To avoid external compression, experts recommend spacing out your lip filler appointments. Instead of injecting a large amount of filler in one sitting, opt for smaller, gradual touch-ups spaced 7 to 14 days apart.
3. Unpredictable Facial Anatomy & Hidden Scars
No two faces are identical. Your superior and inferior labial arteries (the main blood suppliers to your lips) might sit much shallower or deeper than the average person.
Furthermore, previous lip surgeries, trauma, or old filler can create internal scar tissue. Scar tissue is rigid and can anchor blood vessels in place. When a vessel is pinned down by a scar, it cannot naturally slip away from an advancing needle, making an accidental puncture much more likely.
How common is vascular occlusion lip filler?
Vascular occlusion is considered a rare complication. According to various medical studies, the incidence rate is estimated to be around 0.05% to 0.1% (roughly 1 in 1,000 to 1 in 10,000 cases). However, because lip fillers are incredibly popular, cases do occur. The risk heavily depends on the injector’s knowledge of facial anatomy, their experience, and the techniques used.
How to know if you have vascular occlusion lip filler?
Recognizing the signs early is critical. The most common indicators include:
- Severe Pain: Pain that is out of proportion to a normal injection, often described as a throbbing or sharp ache that doesn’t go away. (Note: Sometimes pain is masked if numbing cream/lidocaine is used).
- Blanching: The skin turns completely white or pale immediately after injection because blood is no longer reaching the area.
- Temperature Change: The affected area feels noticeably cooler to the touch compared to the surrounding skin.
- Mottling (Livedo Reticularis): A purplish, lace-like, or net-like pattern appears on the skin.
- Prolonged Swelling or Blistering: Unusual bruising or the formation of tiny white pustules (blisters) in the days following the treatment.
How to check for vascular occlusion lip filler?
Practitioners and patients can perform a simple test called the Capillary Refill Test (CRT):
- Apply firm pressure to the suspect area of the lip with a clean finger for about 3 to 5 seconds until the tissue turns white (blanches).
- Release the pressure.
- Count the seconds it takes for the pink/red color to return.
- Normal: Color returns in 1 to 2 seconds.
- Warning Sign: If it takes 3 seconds or longer (sluggish refill), or if the color doesn’t return at all, it indicates compromised blood flow and potential occlusion.
Small vascular occlusion lip filler
Sometimes, a VO doesn’t block a major artery but rather smaller capillaries (micro-occlusion).
- Symptoms: A small vascular occlusion might not cause massive pain but could show up as a tiny white spot, a persistent small blister, or a localized dark patch that looks like a bad bruise.
- Action: Even small occlusions should never be ignored, as they can lead to localized tissue damage or scarring. They require the same immediate medical assessment as a major occlusion.
Delayed vascular occlusion lip filler
While most vascular occlusions happen immediately during the procedure, delayed occlusions can occur hours or even a few days later.
- Why it happens: Hyaluronic acid (HA) fillers are hydrophilic (they attract water). Over 24-48 hours, the filler expands. If it was placed too close to a vessel, this expansion can create delayed external compression (Extravascular Compression), slowly cutting off the blood supply.
Necrosis vascular occlusion lip filler
Necrosis (tissue death) is the worst-case scenario and the end-stage result of an untreated vascular occlusion.
- If blood flow is not restored, the starved tissue begins to die.
- The area will transition from white/mottled to dark purple, grey, and eventually black and scabbed.
- Tissue necrosis leads to permanent scarring, disfigurement, and the need for surgical reconstruction. This is why VO is treated as an absolute emergency.
How to prevent & avoid vascular occlusion lip filler?
Prevention is always better than cure. To avoid VO, patients must choose highly qualified medical professionals. Safe injection protocols include:
- Thorough Knowledge of Anatomy: The injector must deeply understand the depth and location of the facial arteries (e.g., the superior and inferior labial arteries).
- Aspiration: Pulling back on the syringe plunger before injecting to check for blood return (though not 100% foolproof, it is a common safety step).
- Using Cannulas: A blunt-tipped cannula is less likely to pierce a blood vessel compared to a sharp needle.
- Slow Injection & Low Pressure: Injecting tiny amounts of filler slowly reduces the risk of pushing filler forcefully into a vessel.
- Keeping Filler Moving: Avoiding depositing large clumps of filler (boluses) in one high-risk spot.
How to treat vascular occlusion lip filler?
If an occlusion occurs, the treatment protocol must be initiated immediately:
- Hyaluronidase (Hylenex): This is the “antidote.” It is an enzyme injected directly into the affected area to dissolve the Hyaluronic Acid filler instantly, unblocking the vessel. Multiple high doses may be required until capillary refill returns to normal.
- Warm Compresses & Massage: Applying heat and vigorously massaging the area to encourage vasodilation (widening of blood vessels) and blood flow.
- Aspirin: The patient is often given aspirin to thin the blood and prevent clotting in the restricted vessel.
- Nitroglycerin Paste: Sometimes applied topically to further dilate the blood vessels.
- Follow-up: Daily monitoring by the practitioner to ensure tissue is healing and blood flow remains stable.
The Emergency Protocol: What to Expect at the Clinic
If you show signs of vascular occlusion, your injector must immediately stop the procedure and switch to an emergency rescue protocol. Time is tissue. The faster blood flow is restored, the lower the risk of permanent damage.
The “48-Hour” Golden Window
Medical studies show that if high-dose hyaluronidase (the filler dissolver) is administered within the first 48 hours of an occlusion, the chances of a complete recovery and zero permanent tissue damage are exceptionally high.
The Step-by-Step Rescue Plan
If you are in an occlusion crisis, your provider should immediately perform the following steps:
Step 1: Flood the Area with Hyaluronidase If a hyaluronic acid (HA) filler was used, the injector will rapidly inject high doses of hyaluronidase (often 150 to 500+ units) directly into the blanched and painful areas. This enzyme breaks down the filler plug. They will likely inject it hourly until the pink color returns to your skin.
Step 2: Vigorous Massage and Heat Your provider will apply warm compresses (around 104°F) and firmly massage the area. Heat dilates (widens) the blood vessels, and massage helps disperse the dissolving filler, encouraging fresh blood to push through the blockage.
Step 3: Blood-Thinning Medications You will likely be given a stat dose of oral Aspirin (usually 300mg/325mg) right in the clinic. Aspirin prevents blood platelets from clumping together and forming a secondary clot behind the filler blockage.
Step 4: Vasodilators (Nitroglycerin) Depending on the clinic’s protocol, the practitioner might apply Nitroglycerin paste directly to the skin. This powerful topical medication rapidly forces the local blood vessels to open up, allowing oxygen to reach the starving tissue.
At-Home Monitoring: The First 24 Hours
Even if your procedure went smoothly, vascular occlusion can still develop on a delay (up to 24 hours later). Your post-appointment aftercare is your first line of defense.
How to Monitor Your Lips at Home
- The 15-Minute Rule: Check your lips in a mirror every 15 to 30 minutes for the first two hours after your injection. After that, check hourly for the next 12 to 24 hours.
- Do the Capillary Refill Test: Gently press your finger against the injected area until it turns white, then release. The pink color should return in under 2 seconds. If it takes longer, contact your provider.
- Document Everything: Take clear photos of your lips every few hours in good lighting. If you notice a sudden pale spot, a purple lacy pattern, or expanding bruising, these photos will help your doctor or the ER staff assess the progression of the occlusion.
When to Go to the ER: If you experience sudden vision changes, unbearable pain that painkillers cannot touch, or a rapidly spreading white/purple patch and you cannot reach your injector within 15 minutes, go to the nearest emergency room immediately. Bring your filler product details with you.
Long-Term Recovery & Potential Complications
If a vascular occlusion is caught and treated within the 48-hour golden window, the vast majority of patients heal completely without lasting damage. However, if treatment is delayed, you may face long-term complications.
1. Tissue Necrosis (Skin Death)
If the blood supply is cut off for too long, the starved tissue will begin to die (necrosis). The skin may turn black, form hard scabs, and eventually slough off. Healing from necrosis requires specialized wound care, antibiotics to prevent secondary infections, and strict medical supervision.
2. Scarring and Pigment Changes
Severe tissue injury can leave behind permanent scars, puckering, or skin indentations. The skin may also heal darker or redder than your natural tone.
- Treatment: Once the emergency has passed and the tissue has healed, scars can be improved using silicone gel sheets, laser therapy, or minor surgical revision by a plastic surgeon.
Prevention: How to Choose a Safe Injector
Vascular occlusion is often preventable. As a patient, you have the right to interview your provider before letting them near your face with a needle. Never prioritize a cheap price over medical safety.
Before your procedure, ask your injector these three critical questions:
- “Do you have Hyaluronidase (filler dissolver) in the clinic right now?” If the answer is no, leave immediately. No practitioner should inject filler without the emergency antidote on hand.
- “Are you trained in vascular emergency protocols?” Your injector should be a licensed medical professional (doctor, registered nurse, or dentist) who knows exactly how to handle an occlusion.
- “Do you use a cannula or ultrasound?” Advanced injectors often use blunt-tip cannulas in high-risk areas to avoid piercing vessels. Some even use handheld ultrasound devices to map out your specific facial arteries before injecting.
Frequently Asked Questions (FAQs)
Can vascular occlusion resolve on its own? No. Vascular occlusion is a medical emergency that will not fix itself. Without immediate medical intervention (usually hyaluronidase injections), the blocked blood flow will lead to tissue death and permanent scarring.
How long does it take for vascular occlusion to show up? Symptoms can appear instantly during the injection or develop slowly over the next 12 to 24 hours. This is why strict at-home monitoring during the first day is crucial.
Can all lip fillers be dissolved in an emergency? No. Only Hyaluronic Acid (HA) fillers (like Juvederm or Restylane) can be dissolved using the enzyme hyaluronidase. Biostimulatory fillers or permanent fillers cannot be easily dissolved, making an occlusion much harder to treat.
Is vascular occlusion painful? Yes, it is typically accompanied by intense, sharp, or throbbing pain that is out of proportion to a normal injection. However, if your filler contains lidocaine (a numbing agent), this pain might be temporarily masked for the first hour or two.
What are the early signs and the first stage of vascular occlusion after lip fillers?
The first stage of vascular occlusion usually begins instantly or within a few hours. The main early signs include blanching (the affected skin turning suddenly white or pale), intense and escalating pain that throbs, and a noticeable drop in skin temperature. Another critical early warning is a sluggish capillary refill—if you press the lip, it takes longer than 3 seconds for the pink color to return. (Note: If your filler contained lidocaine, the initial pain might be masked temporarily).
How long does it take for vascular occlusion to appear after fillers?
Vascular occlusion can occur instantaneously while the needle is still in your lip. However, it is also common to experience delayed vascular occlusion after fillers. Delayed symptoms can show up anywhere from a few hours up to 24 hours post-procedure as swelling increases and compresses a nearby vessel. This is why monitoring your lips closely for the first full day is critical.
Lip Occlusion vs Bruise: How can you tell the difference?
It is easy to confuse a bruise with an occlusion, but their behaviors are very different.
- A normal bruise is mildly tender, stays localized to the injection site, and feels soft. When you press a bruise, the color returns almost immediately.
- A lip occlusion is intensely painful and causes the skin to look dusky, white, or develop a lacy purple pattern (livedo reticularis). Crucially, an occlusion shows a delayed capillary refill (taking more than 3 seconds to pink up after being pressed) and the area may feel unusually cold.
What is the vascular occlusion lip filler timeline and the signs of necrosis?
If left untreated, an occlusion progresses rapidly. Here is the typical timeline:
- 0 – 2 Hours (First Stage): Severe pain, blanching (white/pale skin), and slow capillary refill.
- 2 – 24 Hours: The skin develops a mottled, bluish, or lacy purple pattern as deoxygenated blood pools.
- 24 – 72 Hours (Signs of Necrosis): The first signs of necrosis after filler appear. The starved tissue begins to break down, forming small white blisters, pustules, or ulcers on the skin.
- Days Later: The dead tissue turns black or forms a hard, dark scab (eschar), leading to irreversible scarring and tissue loss.
What is the riskiest place for fillers on the face?
The riskiest areas for facial fillers are the glabella (between the eyebrows), the nose, and the upper lip. Upper lip vascular occlusion is a significant risk because the superior labial artery (the main blood vessel supplying the upper lip) runs through this area. Its depth and position vary greatly from person to person. If an injector places the filler too deeply or deposits too large of a bolus, it can easily puncture or compress this vital artery.
This information is for educational purposes only and does not constitute medical advice. Vascular occlusion is a medical emergency. If you are experiencing severe pain, skin whitening (blanching), or unusual discoloration after getting dermal fillers, contact your injector or go to the nearest Emergency Room immediately. Time is critical to prevent permanent tissue damage.
References & Official Resources
To ensure the highest standards of patient safety and medical accuracy, the information in this article aligns with guidelines and research from the following official government and health organizations:
- U.S. Food and Drug Administration (FDA): Dermal Filler Do’s and Don’ts for Wrinkles, Lips and More – Official FDA guidelines detailing the approved uses and serious risks of dermal fillers, including accidental injection into a blood vessel (vascular occlusion).
- National Institutes of Health (NIH) / PubMed Central: Management of Vascular Occlusion Associated with Cosmetic Injectables – A government-backed database providing peer-reviewed clinical studies on emergency protocols and hyaluronidase administration for vascular compromise.
- U.S. National Library of Medicine (MedlinePlus): Cosmetic Injectables and Patient Safety – A trusted federal resource offering patient-focused information on the safety, risks, and emergency warning signs of cosmetic dermal fillers.

Sarah Mitchell is a dedicated aesthetic researcher with over a decade of experience analyzing cosmetic procedures. Obsessed with data and safety, she helps patients to provide real words and navigate the world of lip fillers with verified before and after results and honest cost breakdowns.